Separation of the recti, or stretching of the midline of the abdominal muscles is a common condition after some pregnancies, or after many years of abdominal loading with poor technique, and is called Diastasis Rectus Abdominis.
In some, it can prevent optimal function of the trunk, particularly for rotation tasks.


Do you have a separation or widening of your abdominal muscles in the midline as a consequence of your pregnancies or excessive, inappropriate abdominal training? Are you struggling to progress in your exercise program (core training/strengthening)?
If so, our comprehensive program that begins with a whole body biomechanical, motor control and ultrasound examination to determine the best treatment plan for restoring function of your stretched abdominal wall may be for you.
Watch the two video clips on this page and read the article associated with this condition (see below) and then call us today for a complete examination of your abdominal wall if you feel this condition applies to you.
The following article is adapted from a presentation on Diastasis Rectus Abdominis (DRA) Diane did at the World Congress for Low Back and Pelvic Pain, in Singapore 2016. Diane has added some ‘lay language explanations’ at key points in the article.
DRA – Should we Open or Close the Gap?
Impairments of abdominal wall function have been implicated in multiple conditions associated with pregnancy and delivery including low back and pelvic girdle pain (LB & PGP), urinary incontinence (UI), pelvic organ prolapse (POP) and diastasis rectus abdominis (DRA). The evidence clearly shows a relationship between pregnancy, back pain and incontinence, thoracic posture and pelvic organ prolapse, as well as a strong association of breathing and continence disorders with back pain.
The Australian Longitudinal Study on Women’s Health surveyed 28,000 women and found that pregnant women experienced more back pain than non-pregnant women as well as more incontinence (Smith et al 2008). In a much smaller study, Pool-Goudzwaard et al (2005) note that 52% of women report a combination of LB & PGP together with some form of pelvic floor dysfunction, such as incontinence, sexual dysfunction and/or constipation. Sixty-six percent of women with DRA have at least one support related pelvic floor dysfunction, such as UI, fecal incontinence or POP.
It is well accepted that pregnancy and delivery present huge challenges not only for the pelvic floor but also for the abdominal wall. In addition to LB & PGP, motor control changes of the abdominal wall and DRA are common both during and after pregnancy.
While evidence is limited with respect to the changes in structure and function of the abdominal wall during and after pregnancy, it appears that for some recovery is not spontaneous without intervention. The long-term impact of poor abdominal wall strategies on bowel, bladder and sexual function has not been investigated in a longitudinal study. Clinical observations suggest that suboptimal abdominal wall strategies can impact bowel, bladder and sexual function immediately, and for many years, after pregnancy and delivery.
Pregnancy-related Diastasis Rectus Abdominis
Few studies have investigated the prevalence of DRA during and after pregnancy. Boissonnault & Blaschak (1988) followed 71 primiparous women for one year and note that 66% had a DRA in the third trimester of their pregnancy and that 36% of these remained abnormally wide at seven weeks postpartum. In a much smaller study, Gilleard & Brown (1996) found that 100% of their six subjects showed separation of the recti by 30 weeks gestation. Recently, it has been reported that 100% of women have a DRA by 35 weeks gestation and the separation persists in 40% when measured at six months postpartum (Mota et al 2014).
Coldron et al (2008) followed 115 postpartum women and used ultrasound imaging to measure the separation between the left and right rectus abdominis (known as the inter-recti distance (IRD)) at day one and months two, six and 12. The IRD was wider in all the primiparous women compared to 69 age-matched nulliparous women in all four groups and these values plateaued at eight weeks postpartum not returning to those of the controls at 12 months. Similarly, Mota et al (2014) reported 39.3% of their postpartum subjects had a wider IRD than normal at six months. Liaw et al (2011) found that the resting IRD reduced and that abdominal wall strength improved up to six months postpartum but not to normal values.
What this means is that the distance between your recti muscles is not likely to change much after 8 weeks postpartum unless you do something about it!
The risk factors for developing a DRA during pregnancy that does not resolve postpartum are unclear. Mota et al (2014) found no statistical differences in women with persistent DRA at 6 months postpartum from those without when the following variables were compared:
- pre-pregnancy body mass index
- body mass index at 6 months postpartum
- weight gain during pregnancy
- baby’s birth weight, abdominal circumference during pregnancy
- general hypermobility statistics (Beighton’s Score).
Width of the Linea Alba (LA) – the Inter-Recti Distance (IRD)
In order to define an abnormal width of the linea alba (LA), and thus a diastasis rectus abdominis, it is critical to know what is average, or normal, in healthy nulliparous individuals. In 2009, Beer et al used ultrasound imaging to investigate the width of the LA in 150 healthy, nulliparous women between the ages of 20 and 45. The IRD was measured at three points along the LA: at the xyphoid, 3 cm above the umbilicus and 2 cm below the umbilicus. They found high variability at all three levels and reported the mean width to be 7mm ± 5 at the xyphoid, 13mm ± 7 3cm above the umbilicus and 8mm ± 6 2cm below the umbilicus. Widths wider than these were considered abnormal.
Linea alba behaviour in healthy individuals
The curl-up task has been used in research to assess function of the abdominal muscles as well as the behavior of the LA. During this task, all the abdominals should co-activate and the distance between the left and right rectus abdominis, known as the inter-recti distance (IRD), should not narrow or widen from the rest position.
Diane Lee & Paul Hodges investigated the behavior of the LA during three tasks in two groups. The control group was comprised of 17 men and nulliparous women and the DRA group of 26 women with IRD widths greater than the suggested normal/average values proposed by Beer et al (2009). Ultrasound imaging was used to measure the IRD at two points: the UX – a point ½ way between the top of the umbilicus and the xyphoid and the U – a point just above the umbilicus. In the 17 healthy males and nulliparous females the IRD and behavior of the LA was evaluated during three tasks:
- At rest in the supine hook lying position with arms by sides,
- During a short head/neck curl-up task (just to the level of the spine of the scapula) with no specific pre curl-up instruction (this was called the Auto-CU), and
- During a short head/neck curl-up task with the instruction to activate the deep muscles of the trunk (including the pelvic floor and TrA) prior to performing the curl-up (this was called the TrA-CU).
For this study, Hodges developed a method to quantify any noted distortion (doming, sagging, undulation) of the LA and called this the distortion index (DI). In all 17 healthy subjects, there was no statistical difference in either the IRD or the DI in all three tasks (rest, Auto-CU, TrA-CU) at either the UX or U points of the LA. There was no statistical difference in either the IRD or DI between the men and nulliparous women in the control group for any of the tasks.
This means that at rest you should not be able to sink your fingers deeply into the midline of your abdomen anywhere along its length except at and around the umbilicus, where we all have a soft soft. When you lift your head up off the pillow to your shoulder blades you should feel tension in the midline and not be able to pull the left and right recti apart nor feel sharp edges of the medial border of either muscle.
Inter-recti Distance and Linea Alba Behavior in Individuals with DRA
The response of the IRD during a curl-up, or abdominal crunch, in women with DRA has been reported in the literature with varying interpretations of what the findings suggest for training women with DRA (Lee & Hodges 2016, Pascoal et al 2014, Sancho et al 2015).
In our study, 26 women with DRA were included. Although not formally reported in the paper, each subject’s ability to transfer loads through their trunk during two additional tasks (one leg standing with contralateral hip flexion (OLS) and a supine active straight leg raise (ALSR) was evaluated.
All subjects with DRA in our study were unable to transfer loads optimally through the trunk during one or more of the two functional tasks tested (OLS, ASLR), with one or more body regions (thorax, lumbar spine, pelvis) showing signs of impairment. The region showing the poorest control appeared to be associated with the region of the LA where the IRD was the greatest and the LA most distorted (least amount of palpable/observable tension). This is a clinical observation only at this time since the relationship was not directly analysed in this study.
You may find you have more pain in your upper low back (bra strap level), middle low back or low low back and this often depends on where you are lacking support from your abdominals. Most people with a significant DRA find rotation tasks against resistance difficult and weak.
When women with DRA performed the Auto-CU task, the IRD reduced from resting values (the gap between the left and right recti narrowed) similar to the findings of other published studies. However, what others did not investigate was the change in distortion of the LA during the Auto-CU (the sagging or doming of the LA). We found in this group that the LA became more distorted (domed, sagged or undulated) when the IRD reduced during the curl-up. Our study was the first to report on this aspect of the behavior of the LA in this group. The distortion of the LA was quantified using the distortion index.
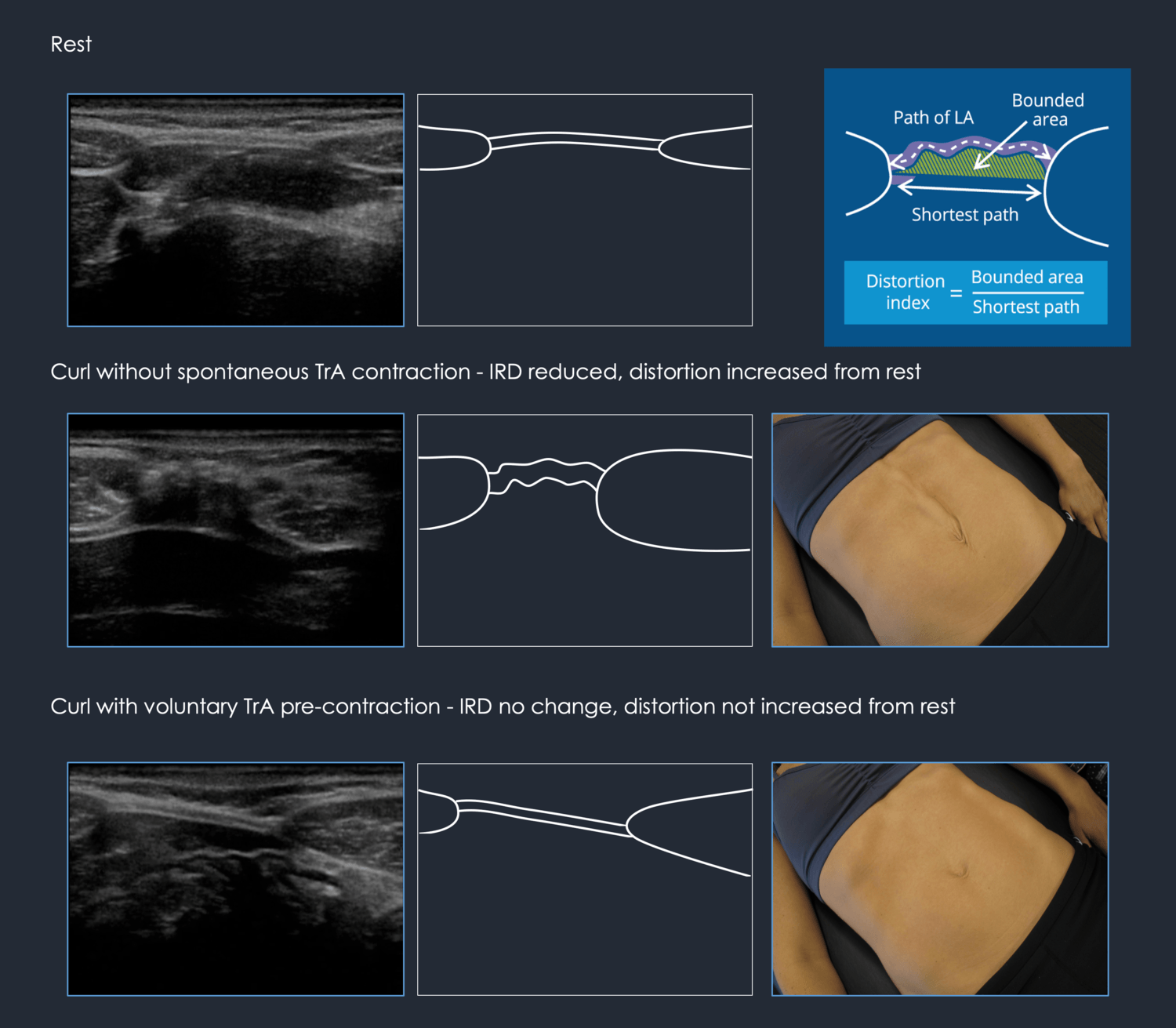
Pre-activation of the transversus abdominis muscle during the TrA-CU (connect to TrA and then curl-up) lessened the reduction of the IRD (IRD widths were larger than those found in the Auto-CU), and reduced the distortion of the LA. Since the IRD did not narrow as much with pre-activation of TrA, this has been interpreted as ‘undesirable’ since the goal in treating women with DRA has focused solely on ‘closing the gap.’ Consequently, clinicians and trainers have been advised to not give exercises that focus on TrA training.
So, transversus abdominis pulls on the sheaths of the recti muscles and then the linea alba thus pulling it wider BUT it also reduces the distortion. In other words the midline doming or sagging was less and the abdomen appears flatter because the TrA muscle is pulling everything in. The goal is not to reduce the gap after all – it is to widen it, load it, and hold the abdominal contents in!
Our interpretation of the changes in IRD when considered with respect to the distortion index is different from other researchers. When the IRD narrows and the LA becomes more lax, we see that there is increased potential for distortion (doming or sagging) when the intra-abdominal pressure increases (see figure above). Not only does this worsen the appearance of the abdomen, it also renders it less effective for transferring loads across the midline. Controlling the reduction of the IRD, with strategies that reduce the LA distortion during a short head/neck curl-up or abdominal crunch, may improve functional and cosmetic outcomes. We suggest that clinicians and trainers should not focus on training strategies that merely reduce the IRD (abdominal crunch without pre-activation of TrA) especially if such strategies increase distortion of the LA. Further clinical studies investigating more variables are needed to resolve the differing opinions.
What this means is that your deepest abdominal, transversus abdominis is important to train IN CONJUNCTION with all the other abdominals as it is this muscle that tenses the linea alba and allows forces to cross the midline – it helps to make you stronger for all rotation tasks! It doesn’t matter that the distance widens as long as you can’t push the tissue into your abdomen in the midline.
Strategies Used to Perform a Curl-up Task in Individuals with DRA
DRA is not limited to postpartum women; it is a condition also seen in men, athletes of both genders and children. Individuals with DRA use a wide variety of strategies to perform a curl-up task and, when assessed in the clinical setting, most strategies are suboptimal in that dys-synergies of the abdominal muscles are present. Similar to LB & PGP, there does not appear to be one consistent dys-synergy common to all individuals with DRA, and therefore there cannot be one treatment program.
In some, there is dominance of the internal oblique muscle (uni or bilaterally) with little, if any, co-activation of external oblique (EO) or transversus abdominis. In others, the EO is the dominant abdominal (uni or bilaterally) with or without co-activation of TrA. The LA can sag dorsally, or invaginate, into the abdominal cavity if the diaphragm is draw up into the thorax as they performed the curl-up. More often, the LA domes if the strategy significantly increases the intra-abdominal pressure. Both strategies (resulting in either invagination or doming of the LA) produce marked distortion and, most often, laxity of the LA.
In many, training pre-activation of TrA prior to the CU eliminates the invagination/doming of the LA, increases tension of the LA, reduces the ability to manually separate the left and right recti and reduces the effort required to perform the short CU task, the OLS and the ASLR. Release of neuromuscular, articular and/or visceral vectors between the thorax and pelvis that cause ‘twists in the trunk’ is often required before symmetric pre-activation of TrA can be achieved. Specific individual muscle training (TrA, dmF, PFM) is not always required after these vectors are released, though sometimes they are. Individual assessment is always necessary to determine next steps in treatment.

There is a subgroup of individuals (more women than men) with DRA in whom the LA can not be tensed nor the distortion reduced in spite of apparent optimal co-activation strategies of all abdominals in multiple tasks. This individual presents with multiple sites of impairment during vertical and horizontal loading tasks, many of which do not improve with manual or verbal corrections of the skeleton. The best correction for this individual is approximation of the left and right recti at the specific level where the LA is widest, most lax and distorted. This is the person with a DRA who should be considered for a surgical plication of the recti and abdominoplasty. If the LA and aponeuroses are able to generate sufficient tension to control the joints of the low thorax, lumbar spine and pelvic girdle through the contraction of the deep muscles, then training will likely be effective for restoring function. If, however, the myofascial system is not able to generate sufficient tension, training will not be effective and surgery is indicated to restore the anatomical integrity.
We can help you to determine if you can train your abdominal wall better or if surgery should be considered. An ultrasound examination is critical for this determination. We can also connect you with good plastic surgeons in the Vancouver area to consult with. But first, come see us to an evaluation!
Summary
Diastasis of the rectus abdominis is a myofascial system impairment of both the linea alba and the left and right recti and has the potential to disrupt mechanisms for transferring load between the thorax, lumbar spine and pelvis. The ability to generate tension and minimize distortion in the linea alba appears more significant for function as opposed to the inter-recti distance. From our initial study (Lee & Hodges 2016), we have acquired considerable knowledge and clinical expertise and are now able to develop a more formal clinical trial to properly address the questions for which we now have hypotheses. First, how wide can the linea alba be before a surgical repair should be considered? It’s doubtful that there is any relevance to the inter-recti distance as long as sufficient tension and minimal distortion can be generated to effectively force close the joints of the abdominal canister. Second, what is the best way to close the DRA and restore function to the trunk?
Closure of the IRD and DRA is not an essential requirement for the restoration of optimal strategies for function and performance. What appears to be essential is the ability to generate tension and minimize distortion between the left and right rectus abdominis and thus fulfill the requirements for control and function of the trunk. Each individual with DRA will require a unique program that considers the specific deficits present within the neuromyofascial system and simple DRA protocols or generic exercise programs will not likely be effective for all.
Acknowledgements
I would like to thank Prof. Paul Hodges for his support and guidance for the research pertaining to the behavior of the linea alba in subjects without and with DRA. Additionally, I would like to thank the Clinical Center of Research Excellence, University of Queensland for providing me with a grant to further the investigation of this condition.
Finally, it is the patients who bring us their stories and challenges that I am indebted to and offer my acknowledgement since these individuals challenge us to find better ways to help them restore the quality of their lives. The clinic and my patients remain my ultimate lab for learning, one patient at a time.
Summary
It is apparent from both the research evidence and clinical experience that the biomechanical, and physiological affects of pregnancy and delivery can have a non-optimal impact on the fascial support system of the abdominal canister. Optimal strategies for function and performance depend on the integrity of the articular, neural, myofascial and visceral systems that can be influenced by psychosocial and systemic physiological factors. Not all women with diastasis rectus abdominis require surgery for restoration of full function; however, some do. If a postpartum woman fails to:
- progress in their exercise program
- regain painfree function
- regain urinary continence, and
has noticeable stretch damage to her abdominal wall associated with a diastasis of the rectus abdominis, a complete biomechanical and ultrasound assessment of the myofascial component of the abdominal canister is warranted. A complete assessment of your abdominal wall function is available at Diane Lee & Associates.
References
Albert HB, Godskesen M, Westergaard J G 2002 Incidence of four syndromes of pregnancy-related pelvic joint pain. Spine 27: 2831
Axer H, Keyserling, D G, & Prescher A 2001b Collagen fibers in linea alba and rectus sheaths. I. General scheme and morphological aspects. The Journal of surgical research, 96(1), 127–134
Axer H, Keyserlingk von D G, Prescher A 2001a Collagen fibers in linea alba and rectus sheaths. The Journal of surgical research, 96(2), 239–245
Beales D J, O’Sullivan P B, Briffa N K 2009 Motor control patterns during active straight leg raise in pain-free subjects. Spine 34(9): 861-870
Beer G M, Schuster A, Seifert B, et al 2009 The normal width of the linea alba in nulliparous women. Clinical Anat. 22(6): 706-711
Bø K, Stien R 1994 Needle EMG registration of striated urethral wall and pelvic floor muscle activity patterns during cough, Valsalva, abdominal, hip adductor, and gluteal muscle contractions in nulliparous healthy females. Neurourology and Urodynamics 13(1): 35–41
Bø, K, Morkved S, Frawley H 2009 Evidence for benefit of transversus abdominis training alone or in combination with pelvic floor muscle training to treat female urinary incontinence: A systematic review. Neurourology and Urodynamics 28(5): 368-373
Boissonault J S, Blaschak M J 1988 Incidence of diastasis recti abdominis during the childbearing year. Physical Therapy 68(7):1082
Chiarello C M, McAuley J A, Hartigan E H 2016 Immediate Effect of Active Abdominal Contraction on Inter-recti Distance. Journal of Orthopaedic and Sports Physical Therapy 46(3): 177–183
Coldron Y, Stokes M J, Newham D J et al 2008 Postpartum characteristics of rectus abdominis on ultrasound imaging. Manual Therapy 13: 112
Gilleard W L, Brown J M 1996 Structure and function of the abdominal muscles in primigravid subjects during pregnancy and the immediate postbirth period Physical therapy, 76(7): 750–762
Gräßel D, Prescher A, Fitzek S, Keyserlingk D G V, Axer H 2005 Anisotropy of human linea alba: a biomechanical study The Journal of surgical research, 124(1): 118–125
Guimberteau J-C, Armstrong C 2015 Architecture of human living fascia. Handspring Publishing, Edinburgh
Hungerford B, Gilleard W, Lee D 2004 Altered patterns of pelvic bone motion determined in subjects with posterior pelvic pain using skin markers. Clinical Biomechanics 19(5): 456–464
Larsen E C, Wilken-Jensen C, Hansen A, Jensen D V, Johansen S, Minck H, Wormslev M, Davidsen M, Hansen T M 1999 Symptom-giving pelvic girdle relaxation in pregnancy. I: Prevalence and risk factors, Acta Obstet Gynecol Scand 78: 105-110
Lee D 2015 Highlights from an integrated approach to the treatment of pelvic pain and dysfunction. Ch. 17 in: Magee D J, Zachazewski J E, Quillen W S, Manske R C (eds) Pathology and intervention in musculoskeletal rehabilitation, 2nd edition Edinburgh, Elsevier
Lee D 2016 Diastasis Rectus Abdominis – A clinical guide for those split down the middle. learnwithdianelee.com
Lee D G, Hodges P W 2016 Behaviour of the linea alba during a curl-up task in diastasis rectus abdominis: an observational study. JOSPT (accepted)
Liaw L J, Hsu M J, Liao C F, Liu M F, Hsu A T 2011 The relationships between inter-recti distance measured by ultrasound imaging and abdominal muscle function in postpartum women: A 6-month follow-up study Journal of Orthopaedic and Sports Physical Therapy, 41(6): 435–443
Mattox T F et al 2000 Abnormal spinal curvature and its relationship to pelvic organ prolapse. Am J Obstet Gynecol 183(6): 1381-4
Mens J M, Vleeming A, Snijders C J, Stam H J, Ginai A Z 1999 The active straight leg raising test and mobility of the pelvic joints. European Spine Journal 8(6): 468–473
Mota P G, Pascoal A G, Carita A I, Bo K 2014 Prevalence and risk factors of diastasis recti abdominis from late pregnancy to 6 months postpartum, and relationship with lumbo-pelvic pain. Man Ther 2014; doi: http://dx.doi.org/10.1016/j.math.2014.09.002
Neumann P, Gill V 2002 Pelvic floor and abdominal muscle interaction: EMG activity and intra-abdmominal pressure. International Urogynecology J 13: 125
O’Sullivan P B, Beales D J 2007 Changes in pelvic floor and diaphragm kinematics and respiratory patterns in subjects with sacroiliac joint pain following a motor learning intervention: a case series. Manual Therapy 12(3): 209–218
O’Sullivan P B, Beales D J, Beetham J A, et al 2002 Altered motor control strategies in subjects with sacroiliac joint pain during the active straight-leg-raise test. Spine 27: E1-8
Östgaard HC, Andersson GJ, Karlsson K 1991 Prevalence of back pain in pregnancy, Spine 16: 549-552
Östgaard HC, Zetherström G, Roos-Hansson E 1996 Regression of back and posterior pelvic pain after pregnancy, Spine 21: 2777-2780
Parker M A, Millar L A, Dugan S A 2009 Diastasis Rectus Abdominis and Lumbo‐Pelvic Pain and Dysfunction‐Are They Related? Journal of Women’s Health Physical Therapy 33(2): 15
Pascoal A G, Dionisio S, Cordeiro F, Mota P 2014 Inter-rectus distance in postpartum women can be reduced by isometric contraction of the abdominal muscles: a preliminary case-control study. Physiotherapy 100: 344–8
Pool-Goudzwaard A, Slieker ten Hove M C, Vierhout M E et al 2005 Relations between pregnancy-related low back pain, pelvic floor activity and pelvic floor dysfunction. Internation Urogynecology J Pelvic Floor Dysfunction 16(6): 468
Sancho M F, Pascoal A G, Mota P, & Bø K 2015 Abdominal exercises affect inter-rectus distance in postpartum women: a two-dimensional ultrasound study. Physiotherapy 101(3): 286–291
Sapsford R R, Hodges P W 2001 Contraction of the pelvic floor muscles during abdominal maneuvers. Archives Physical Medicine & Rehabilitation 82: 1081
Sapsford R R, Hodges P W, Richardson C A et al 2001 Co-activation of the abdominal and pelvic floor muscles during voluntary exercises. Neurourology and Urodynamics 20: 31
Smith M D, Coppieters M W, Hodges P W 2007 Postural response of the pelvic floor and abdominal muscles in women with and without incontinence. Neurourology and Urodynamics 26(3): 377
Smith M D, Russell A, Hodges P W 2006 Disorders of breathing and continence have a stronger association with back pain than obesity and physical activity. Australian Journal of Physiotherapy 52: 11
Smith M D, Russell A, Hodges P W 2008 Is there a relationship between parity, pregnancy, back pain and incontinence? International Urogynecology Journal and Pelvic Floor Dysfunction 19(2): 205–211
Spitznagle TM Leong FC Van Dillen 2007 Prevalence of diastasis recti abdominis in a urogynecological patient population. International Urogynecology Journal Pelvic Floor Dysfunction 18(3): 321
Stuge, B, Mørkved S, Dahl H H, Vøllestad N 2006 Abdominal and pelvic floor muscle function in women with and without long lasting pelvic girdle pain. Manual Therapy 11(4): 287–296
Thompson J A, O’Sullivan P B, Briffa N K et al 2006 Altered muscle activation patterns in symptomatic women during pelvic floor muscle contraction and valsalva manouevre. Neurourology and Urodynamics 25: 268
Williams P L 1995 Gray’s anatomy, 38th edn. Churchill Livingstone, New York
Wu W H, Meijer O G, Uegaki K et al 2004 Pregnancy-related pelvic girdle pain (PPP), I: Terminology, clinical presentation, and prevalence. European Spine J 13(7): 575
Further reading and a lecture:
Diastasis Rectus Abdominis – A Clinical Guide for Those Who are Split Down the Middle
Diane also does teleconsults via ZOOM for patients with DRA who are unable to get to the clinic for a complete evaluation. Call the clinic at 604 538 8338 to organize a ZOOM consult. You will be asked to email us the details of your condition plus 3 videos:
1. standing abdominal profile with your abdomen completely relaxed and then with your deep system engaged
2. supine curl-up task without pre-contracting your deep system
3. supine curl-up task with a pre-contraction of your deep system
These videos can be emailed to info@dianeleephyio.com via We Transfer for free. Diane will look at the videos and read your information prior to your initial Zoom consult, which will be recorded for your future reference.
Related Services


The Integrated Systems Model
This model allows clinicians to be more effective and efficient with their assessment and treatment in order to help patients develop better movement strategies and habits to help reduce symptoms and improve function and performance.

Ultrasound Imaging
Ultrasound imaging is useful as a biofeedback tool for ‘rewiring the brain’ or re-educating the proper timing of muscle contraction during both individual exercises and meaningful task training.

Prenatal and Postpartum Screening
There are many myths around pregnancy. Physiotherapists who specialize in pre/post natal care can help debunk these myths, playing an important role in the management of physical changes that can occur both during and after these nine months.



